2301 Ford Street | Golden, CO |
303-278-20/20
About Us
Doctors and Staff
Optical Boutique
Advanced Vision and Eye Testing Instruments
Your eyes
Eyes & Eye Diseases
Eyeglasses
Contact Lenses
Order Contact Lenses Online
All about contacts
Getting contacts
Types of Contacts
Reviews
Recipes for Eye Health
Reviews »
About Us
Doctors and Staff
Optical Boutique
Advanced Vision and Eye Testing Instruments
Your eyes
Eyes & Eye Diseases
Eyeglasses
Contact Lenses
Order Contact Lenses Online
All about contacts
Getting contacts
Types of Contacts
Reviews
Recipes for Eye Health
Reviews »
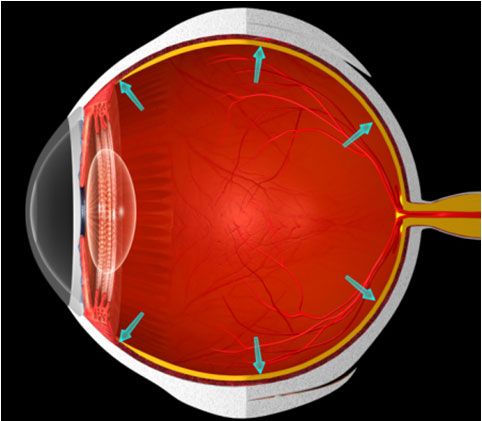
glaucoma